

Dementia
Dr. Manjit Singh


What is dementia? Why is it so important? What are the types? How do we work it up? How do we treat?

Definition of Dementia
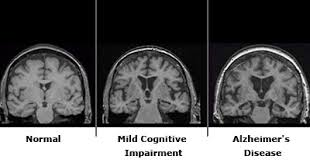
Spectrum of brain disorders, all of which involve cognitive impairment, resulting in significant impairment in daily functioning.

Definition of Dementia
Spectrum of brain disorders, all of which involve cognitive impairment, resulting in significant impairment in daily functioning. Cognitive Function?

Definition of Dementia
Spectrum of brain disorders, all of which involve cognitive impairment, resulting in significant impairment in daily functioning. Cognitive Function? amnesia, aphasia, apraxia and agnosia (the 4 As of Alzheimer's)

Definition of Dementia
Spectrum of brain disorders, all of which involve cognitive impairment, resulting in significant impairment in daily functioning. Associated features Personality changes, disruptive behavior, apathy Depression, psychosis, anxiety, sleep disturbances

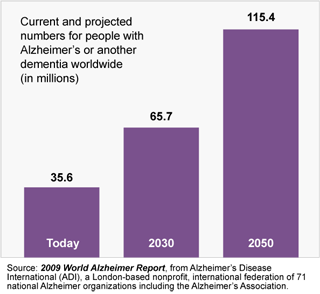
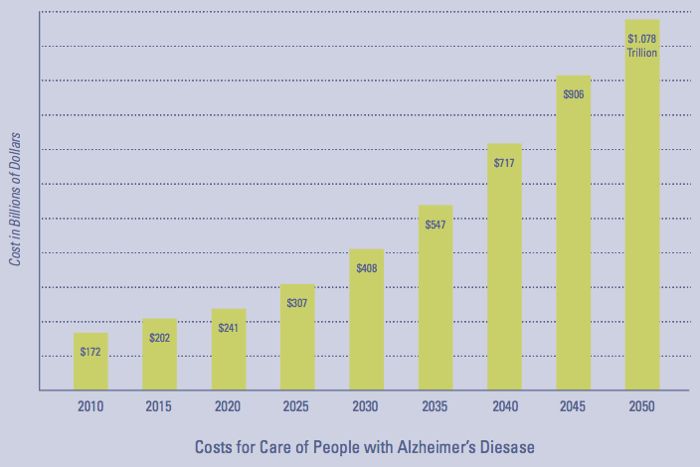
Epidemiology
35 million dementia worldwide 4million Severe dementia in US Annual cost of treating (2010) Dementia-109 billion Heart Disease -102 billion Cancer - 77 billion (Michael D. Hurd, PH.D. et al; NENJM 368;14)

Dementia Subtype, grouped by etiology
Cortical degeneration AD, Lewy body dementia, FrontoTemporal Dementia Subcortical degeneration PD Cerebrovascular vascular dementia Structural or traumatic tumor, paraneoplastic, postanoxic, postop Toxic ETOH, copper, metal, toxic gas exposure Nutritional VitB12, folate, niacin, Thiamine

Dementia Subtype, grouped by etiology
Infectious syphilis, HIV, encephalitis, prion disease Organ failure Uremic/ hepatic encephalopathy Endocrine DM, Hypothyroid, Addison ds, cushing ds. Neurologic/metabolic Huntington disease, Fragile X syndrome Inflamattory SLE, Sjogren, PAN

Dementia Subtype

Dementia Diagnostic Work Up

Dementia Work Up
History of Impairment When it began? What triggered? How it progressed? Describe the specific impairment Evaluate activity of daily living Medical history Psychiatric history Medication Asking same questions to family or care giver is often necessary.

Dementia Work Up
Assessment of the Home Environment Any risky behaviors? Is home safe? Any sign of abuse, neglect, exploitation? What are caregiver’s mental and physical states?

Dementia Work Up
Physical Exam Neurologic Exam Psychiatric Exam Cognitive Screen Depression screening

Cognitive Screening
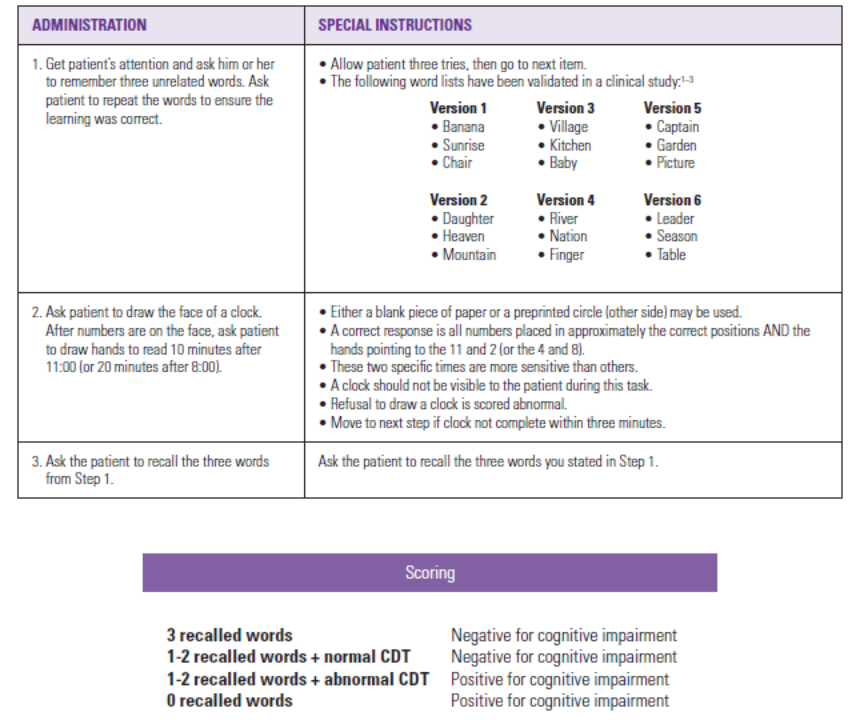
standardized instruments to assess all cognitive domains Mini-Cog (3-item recall + CDT) MOCA, SLUMs, Mini Mental (Foulstein test) Also good for follow up. Avr.2-4 points down per year.


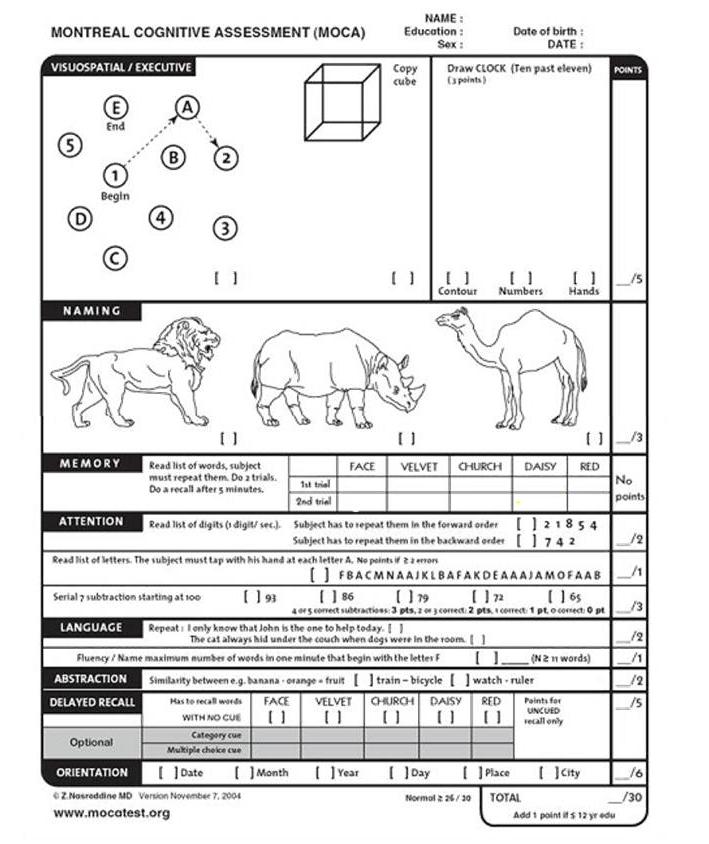
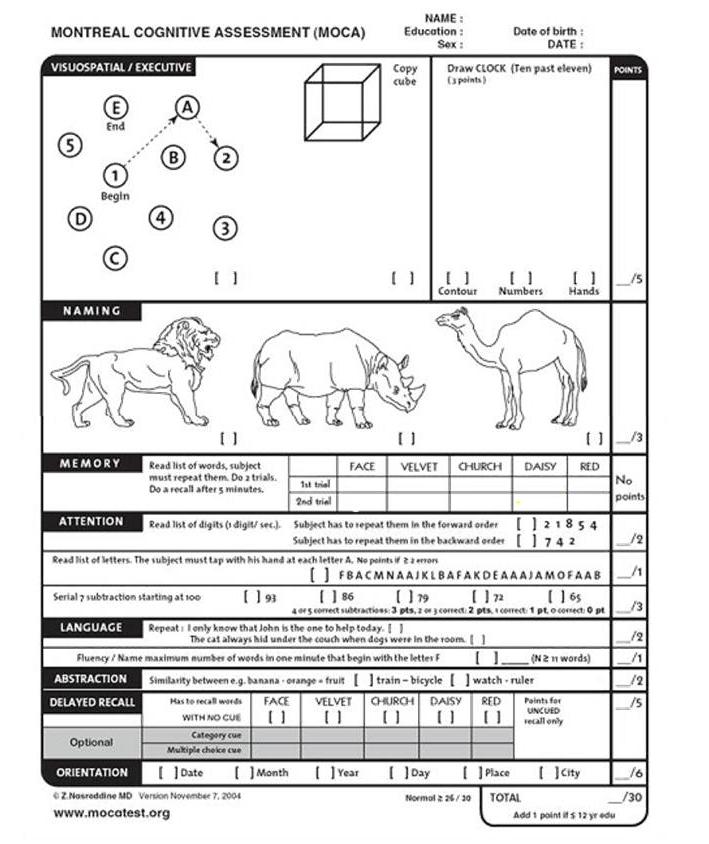
MOCA (Montreal Cognitive Assessment)
Good tool to detect MCI Sen 90%, spec 87% for MCI Sen 98%, spec 87% for Early AD 35 languages, 3 English ver. >25 normal 20 – 25 MCI <20 Dementia


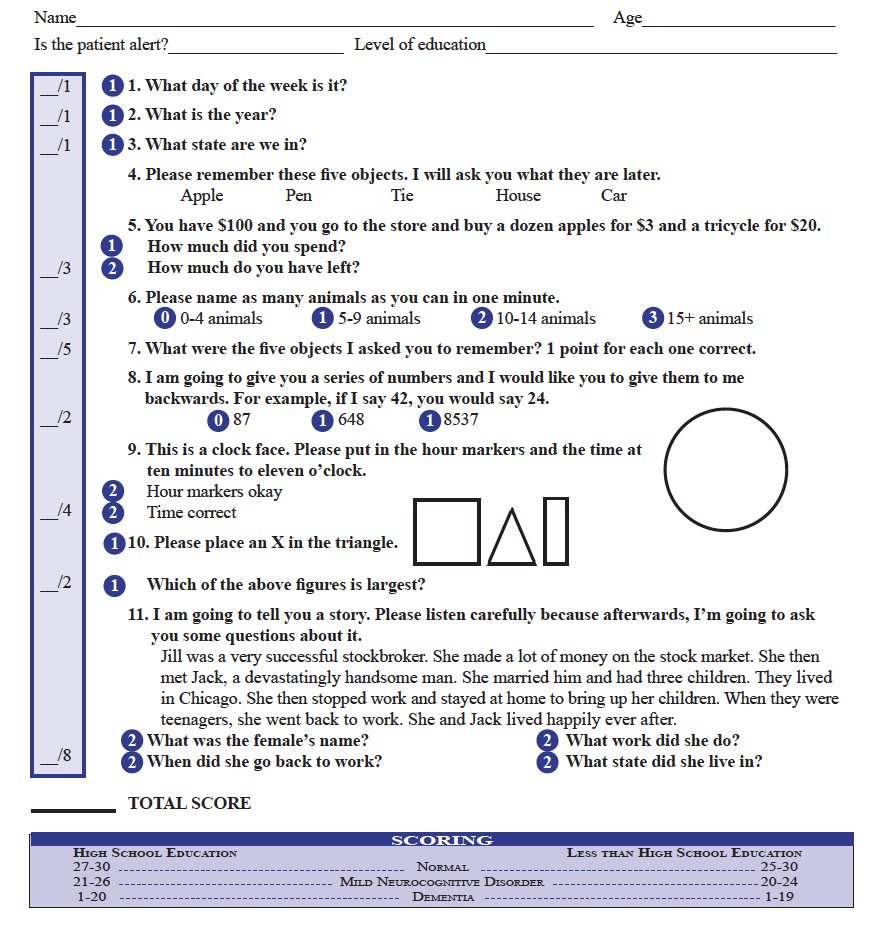
SLUMS (St. Louis University Mental Status Exam)
Design to catch early stages of dementia Sensitivity 92% Specificity 81% for detecting early dementia Adjusted cut-off score per educational level

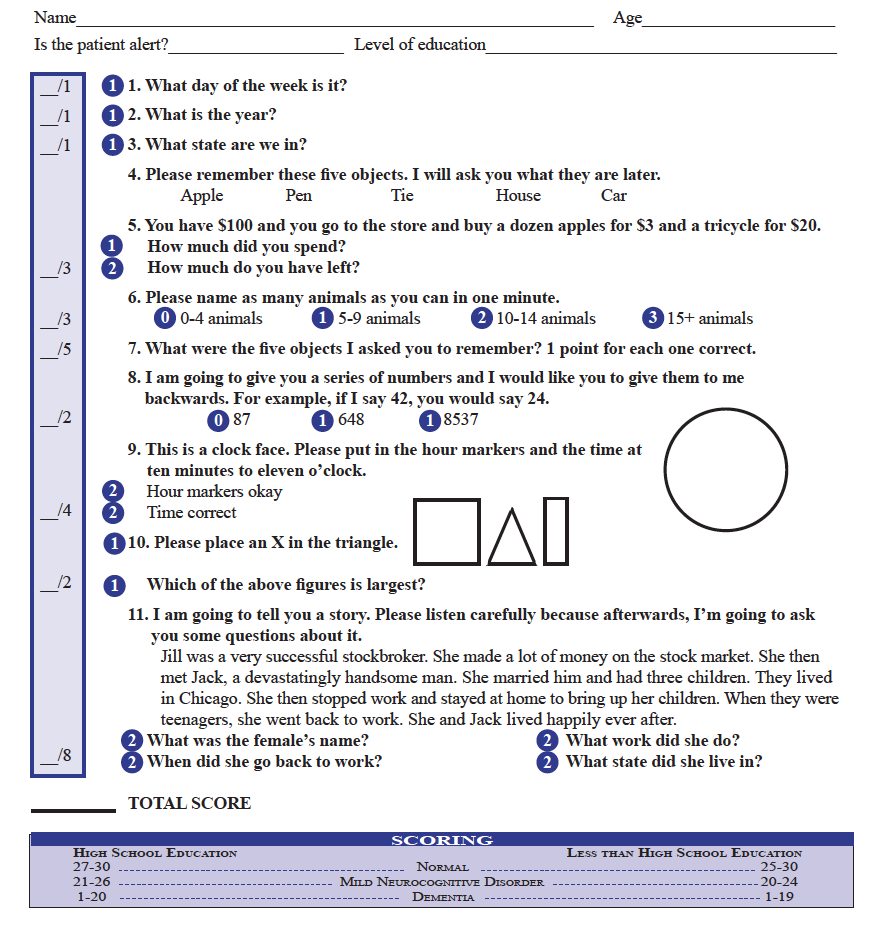

CDT ( Clock Drawing Test)
Simple and easy Assess multiple domains Memory, language comprehension, visuospatial, visuomotor, concentration, executive function, fine motor skill, mathematical *3-point scoring method 1- clock face 2- numbers in correct position 3- hand in correct position

CDT 10-point scoring method
Clock face 0 absent 1 incomplete, some distortion 2 intact Numbers on the clock 0 hardly placed 1 missing or added number, major distortion 2 missing or added number, spatial distortion 3 numbers presents, but spatial distortion 4 numbers all present & correct
Hands of the clock 0 no hand or distorted 1 one hand or distorted two hands 2 both hands present, but misplaced 3 minor error, hour/minute hand same appearance 4 correct placement and size 9-10 normal <7 severe impairment
CDT


Dementia Work Up
Laboratory Tests CBC, CMP, TSH, Vit B12, Folate, RPR, UA Toxicology screen and heavy metal screen, if suspected Neuroimaging of Brain CT, MRI, PET

Dementia Work Up
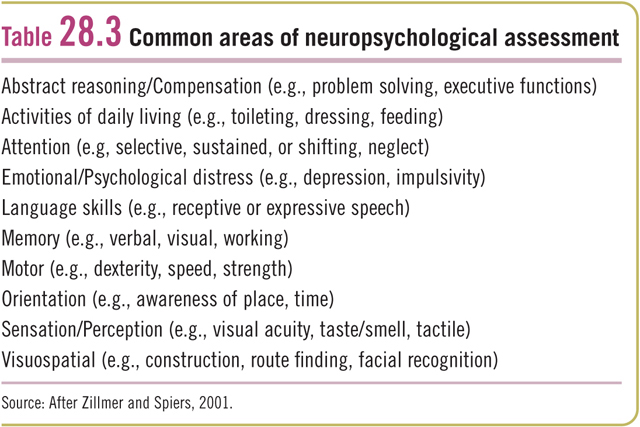
EEG To look for focal lesions and seizure activity EEG in dementia- Diffuse slowing of brain activity, inc.delta And theta frequency. Neuropsychological Testingspecifically designed test to measure psychological function known to be linked to a particular brain structure or pathway

Neuropsychological Testing
Diagnose the presence of cortical damage and localize it if possible Facilitate patient care Identify mild disturbances Identify unusual brain organization Identify the cause of disorders Rehabilitation Help the patient and their family understand the disorder


Importance of early diagnosis
To identify and treat reversible medical causes To establish a diagnosis of dementia to explain To allow the individual to make critical life decisions (financial planning, POA, advance directives, life plans) To maximize safety set limits on driving, hunting, firearms, caring for children To provide treatment to slow the progression or to ameliorate the symptoms to improve quality of life

Case 1.
72 y/o F with history of HTN, urinary incontinence, OA presented with increased forgetfulness that started several months ago. She occasionally forgets doctor’s appointment and misses due dates on her bills. Hence, she is making notes on her pocketbook calendar and carries it with her all the time. She also has difficulty finding words during conversation, gets embarrassed when people are staring at her, waiting for her to say next word. She lives with her husband in a two story house with large back yard, and enjoys gardening. She is a retired school teacher, currently teaches 1stgraders at Sunday school at local church. 140/80, 72 bpm. Physical exam unremarkable MOCA 23/30

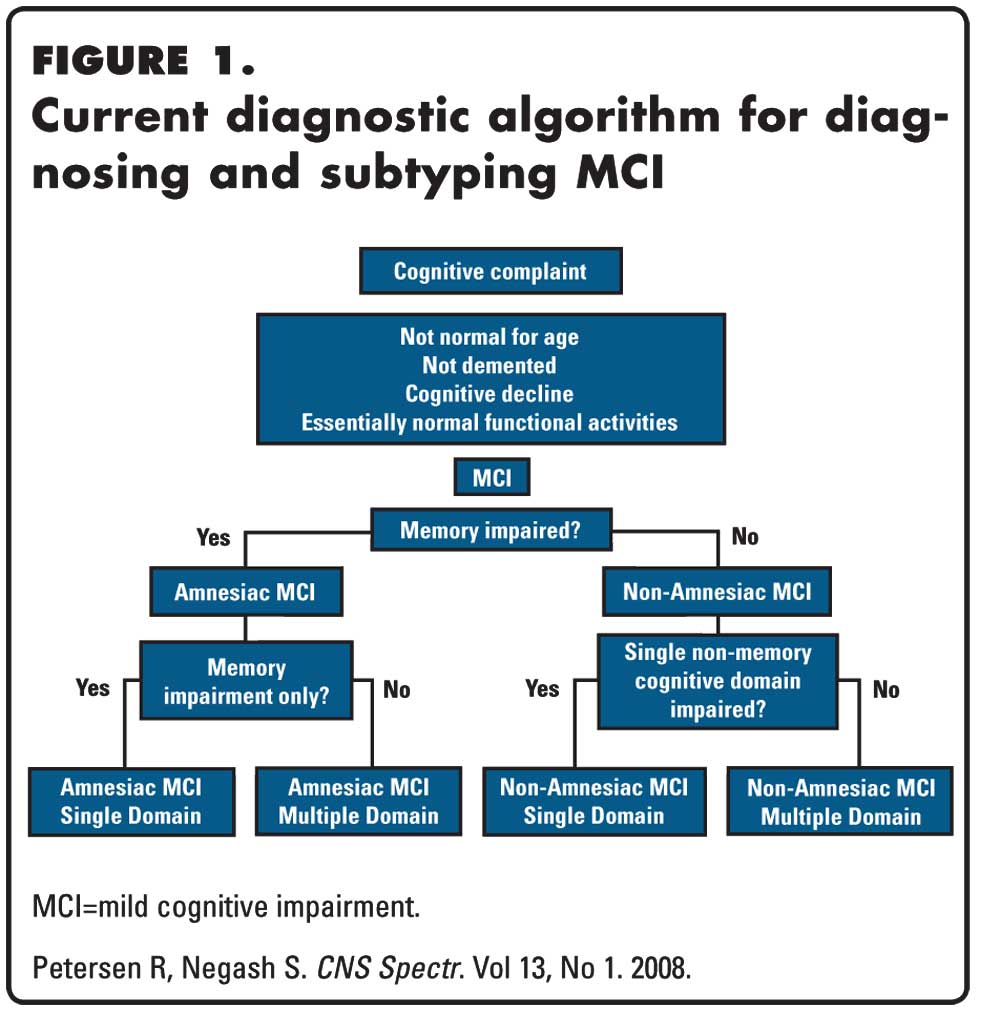
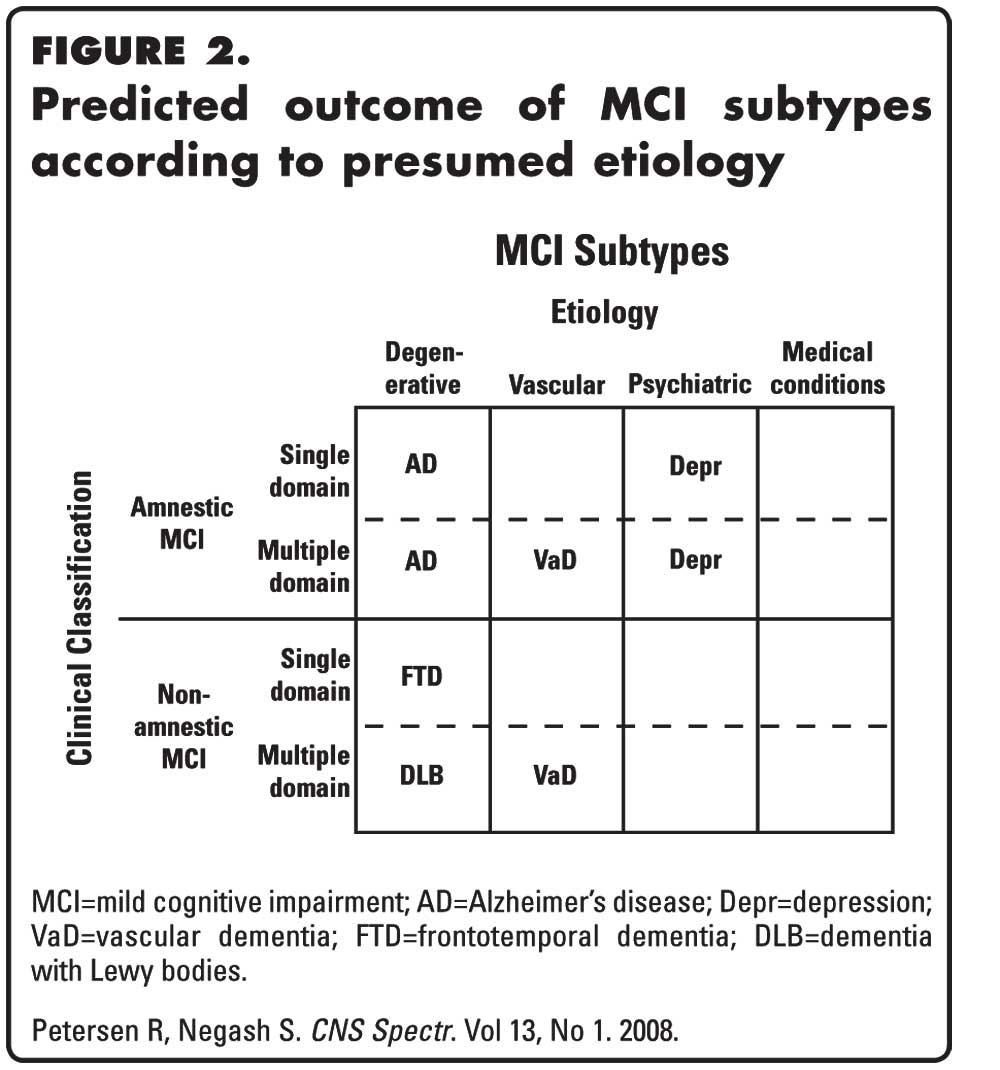
MCI (Mild Cognitive Impairment)

MCI
Syndrome of cognitive declinemore than normalage-associated changes, butless than dementia MCIAD 12-18% / yr vs. Normal AD 1-2 % / yr Original Criteria 1) Memory complaint 2) Memory impaired for age 3) Normal general cognitive function 4) Normal activities of daily living 5) Not demented



Case 2.
69 y/o female with history of HTN, chronic back pain, came to your office, accompanied by her son, who is concerned about mom’s memory. He says that mom was completely normal until three months ago. Now, she is unable to keep her appointments. She often skips meals, forgets taking medications, spends her time sitting in her recliner all day long. However, last week, when her oldest grand daughter visited her from Florida, she cooked the finest Italian dish for her. She drives without problem. Physical exam is unremarkable. She scored 12/30 on MOCA. She seemed not concerned about the score. She did well on CDT and other visuosptial test. She missed points on word recall, serial seven, language, most of the questions, she answered “I don’t know”

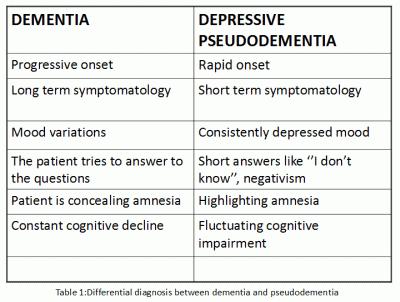
Pseudodementia
Syndrome in which dementia is mimicked by functional psychiatric disorder Depression, schizophrenia, mania, dissociative disorder, conversion disorder Depressive pseudodementia is the most common type

Dementia vs. Pseudodementia

Case 3.
A 75-year-old man with h/o HTN, BPH, Chronic back pain came to your office for initial visit. He feels great, denies any problems other than chronic back pain. However, his daughter is concerned of his memory. Per daughter, he has a 3-year history of progressive memory loss, mainly short- term memory. He needed his daughter to remind him of his appointments and taking medications. He had problems with driving alone as he became confused with the routes, near his house. Daughter recently picked up some mistakes on his check books. When asked, he says that he is getting old and having senior moments. BP 125/70 66bpm, physical examination was unremarkable. MOCA was 19 out of 30.

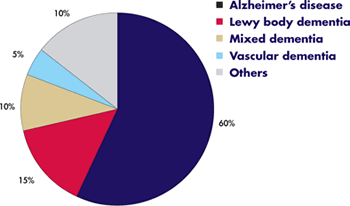
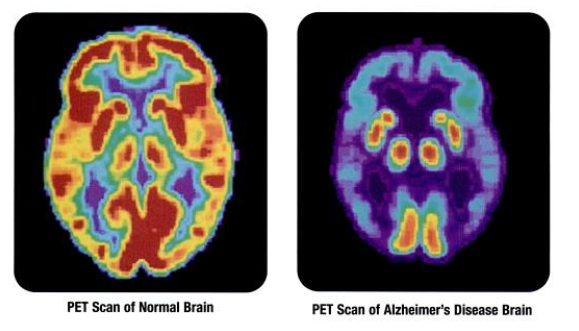
Alzheimer Disease (AD)

AD
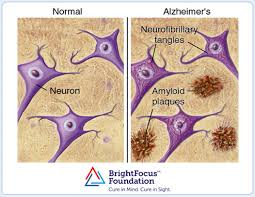
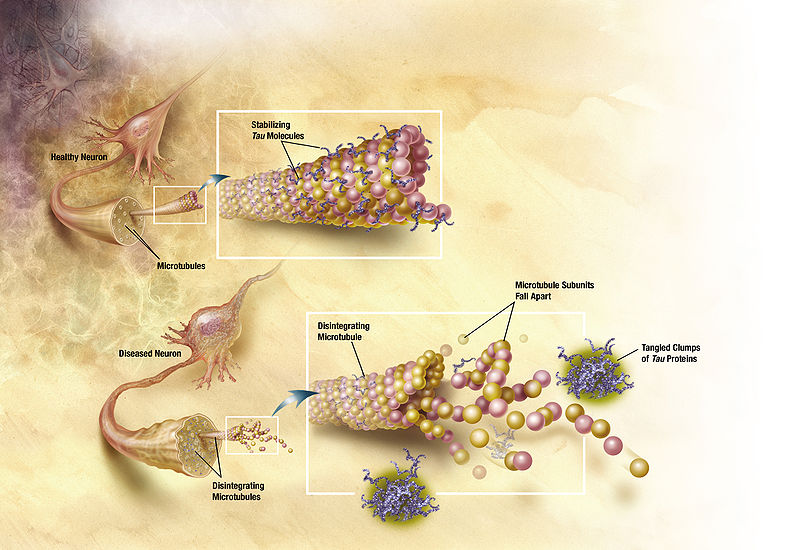
The most common form of dementia (60~70%) 5 million people in US. At age 65: 10% AD at age 85 : 35%Extraneuronal deposition ofbeta-amyloidprotein Intraneuronal destabilization oftau protein-->neurofibrillary tangle

AD

AD
Major Risk factors advanced age (mostly >65), female, menopause, brain injury, presence of apolipoprotein Ee4, family hx. Other risk factorsMedical illness (HTN, DM, CVA, HLD, inc homocysteine) Psychiatric ilness (chronic stress, depression, MCI) Life style(dec. exercise, mental stimulation, active social relationships) Dietary (high fat, high calorie)?

Early onset AD
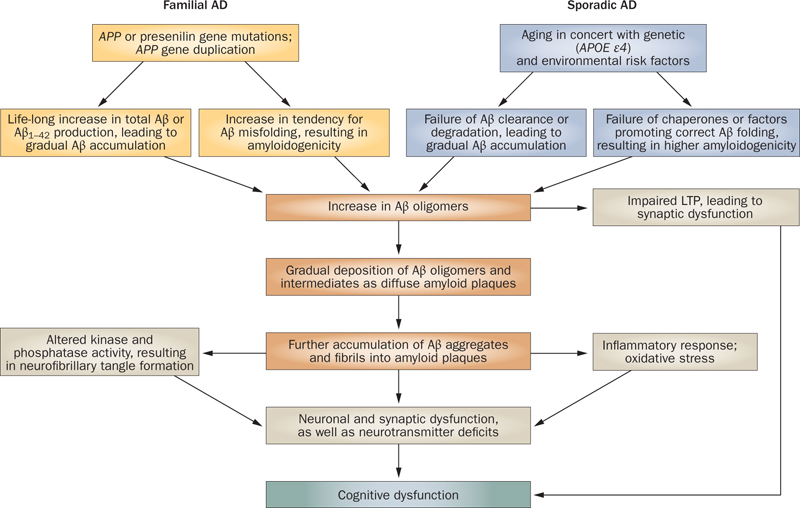
Occurs before age 65 (Usually between 50 to 65) 5-10% of the AD 13% of early onset AD is Familial AD Familial AD caused by mutation in one of at least three genes; Presenilin1, Presenilin2, APP, which are associated with increased level of beta amyloid. Inherited Autosomal Dominant fashion

Beta Amyloid Cascade Hypothesis

NINCDS-ADRDA criteria (1984)
National Institute of Neurological and Communicative Disorders and Stroke and Alzheimer’s Disease and Related Disorders Association Probable AD-progressive deficit in two or more areas of cognitionincluding memory, onset 40-90, absence of other disordersthat can cause cognitive decline Possible AD-A dementia syndrome with atypical feature or progression and without a known etiology. Definite AD-Meets criteria for probable AD and has histopathologic evidence of AD on autopsy or biopsy

NIA-AA (2011)National Institute of Aging and the Alzheimer’s Association
Updated NINCDS-ADRDA criteria 1)Do not require memory impairmentfor AD Impairment of any of 2 or more domain 2) 3 stages PreclinicalNo symptom. (+)Biomarker (CSF beta amiyloid, CSF tau, PET scan ) Predementia(MCI) – Cognitive impairment only DementiaCognitive impairment + compromized function

Treatment of AD
A. All should be engaged in nonpharmacologic approaches that can enhance mental and physical health Eating a well balanced diet rich in fruits & vegetable Mentally and socially stimulating activities Physical exercise - 150minutes per week B. Protect further brain damage by maximizing control of vascular risk factors (HTN, DM, HLD, obesity, smoking) C. Consider pharmacologic agent

FDA approved medication
AChE inhibitors Donepezil (Aricept), Rivastigmine (Exelon), Galantamine Formild, moderate, severe dementia Improve and/or stabilize cognition for 10 to 12 months, followed by a long-term decrease in the degree of symptomatic decline, improve functional abilities Side effect Nausea, Vomiting, Diarrhea, increased gastric acid,syncope, bradyarrhythmia

FDA approved medication
NMDA receptor antagonist Memantine (Namenda) For Moderate to severe stage Can be monotherapy or combined with AChE inhibitor Improve or stabilize cognition, function Side effect : sedation and/or confusion (mild/transient)

Case 4.
A 65 y/o M, with HTN, DM, developed sudden left sided weakness, dysarthria 6 months ago, and was diagnosed with acute right MCA infarct. He was then discharged to rehab. After 8 weeks of intensive rehab, pt almost came back to his baseline. Three months later, his wife noticed that he could not name the only two grand children, and he forgot to take his medications for several days. He could neither operate a remote control nor cook meals as usual. On examination, there was only slight pronator drift on his left arm and hyperreflexia of the left extremities. Scored 17/30 on MOCA

Vascular Dementia

Vascular Dementia
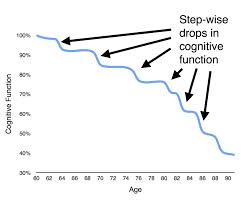
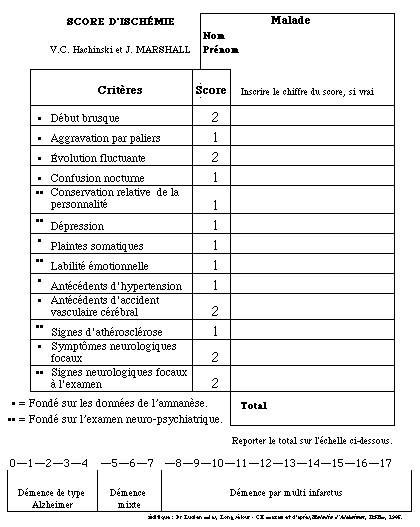
Caused by brain damage due to strokes (thrombotic, embolic, hemorrhagic, lacunar) Dx: Dementia + evidence of CVD Evidence- Neurologic sx, or +neuroimaging Dementia within 3months after stroke Abrupt onset or stepwise progression gait, urinary sx, personality, executive func.
Vascular Dementia

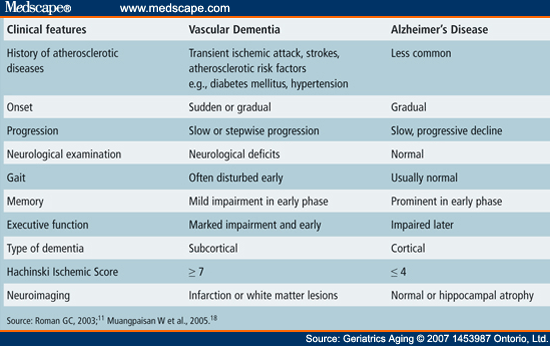
VD vs. AD


Treatment
Primary prevention of stroke in high riskLife Style : Exercise, diet, dec. Obesity, smoking Control BP and glucose level Anticoagulation if +chronic arrhythmia Secondary prevention in pt already affected Anti PLT, Carotid endarterectomy Consider using AChE inhibitor or NMDA antagonist

Case 5.
A 72 y/o M. with a 6-month history of forgetfulness presented to an ER after repeated falls a few days ago. His wife felt that he had been slow in thinking, speaking, and performing his routine activities for a few months. In ER, he was noticed to be confused and hallucinating, hence Haldol was given. After receiving Haldol, he developed significant somnolence and rigidity that lasted 24 hours. After hospitalization, pt slowly improved and now he is at his baseline. On examination, he has bilateral rigidity, and he appears to have flat facial expression.

Dementia with Lewy Bodies

DLBs
Progressive dementia characterized byfluctuating cognitive symptoms, visual hallucinations, andparkinsonism. Second most common Dementia after AD Pathologic hallmark- + abnormal intracytoplasmic protein deposits called Lewy bodies (LBs) DDX: PD associated with dementia- dementia usually occurs later than 1 year, no fluctuation, responds well to Dopaminergic agent
DLBs Diagnosis
The presence of dementia At leasttwoof three core features fluctuatingattention and concentration recurrent well-formedvisual hallucinations parkinsonianmotor signs. C. Suggestive clinical features -Rapid eye movement (REM) sleep behavior disorder -Severe neuroleptic sensitivity -Low dopamine transporter uptake in basal gangliaSPECT or PET imaging Probable DLB: A + 2 Bs or A + 1B + 1C ( sen 83%, spe 95% )

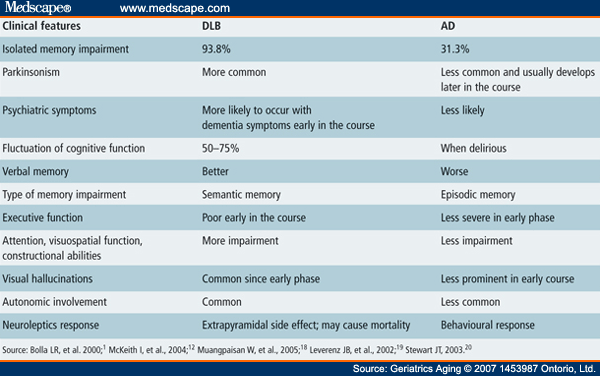
DLB vs. AD

Treatment of DLBs
AChE inhibitor or NDMA antagonist may benefit. Some pt get worse with above medications. Generally start at lower dose, titrate slower than in AD Avoid antipsychotic! Low doses of mood stabilizer or antidepressant can be used for behavior and sleep problems.

Case 6.
A 50-year-old woman presented with behavioral change over the course of two years. She had less concentration to accomplish her assigned tasks and was less responsible to her job. She had begun eating more and had gained 20 pounds in 5 months. She told lies and dirty jokes, stole office stationary, and picked up objects within reach and sight. She had poor personal hygiene and refused to take a bath. Physical exam was unremarkable. Her MOCA was 24/30, but her performance on the clock drawing test was poor.

Frontotemporal Dementia

FTD
1 to 5% of dementia In early onset dementia- 12 – 22% Characterized by the early development ofprominent behavioral symptomsandlanguage disturbances, often before the advent of cognitive disturbances Behavioral disturbances include compulsive behaviors, bizarre delusions, hypersexual behaviors, apathy, unusual oral habits, and inappropriate social conduct. Average survival 6 to 8 years
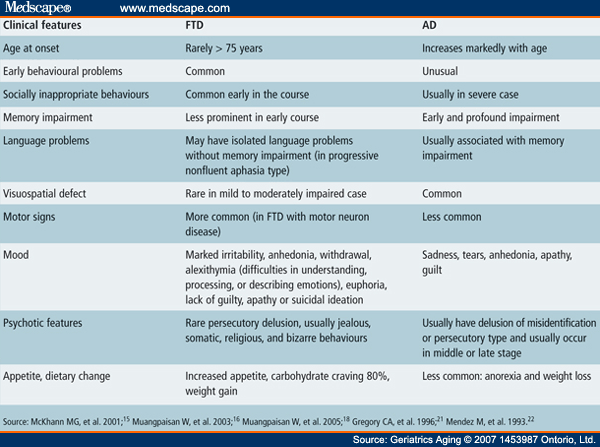
FTD vs. AD

FTD
Treatment focuses on managing symptoms, primarily those affecting behavior. Antidepressants and antipsychotic drugs are the chief medications used to treat behavioral FTD symptoms. None of these drugs have been approved by FDA for use in FTD.

Behavioral Disturbances in Dementia

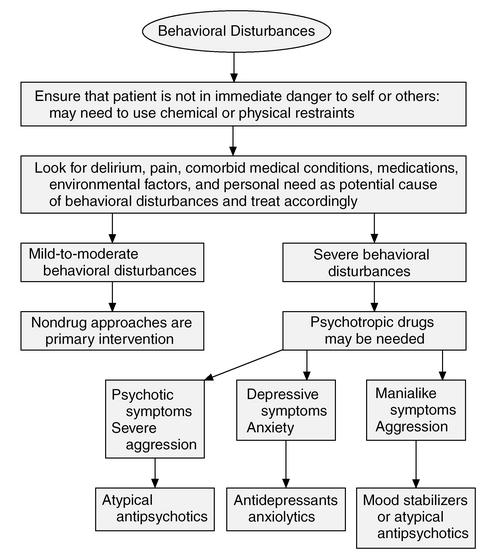

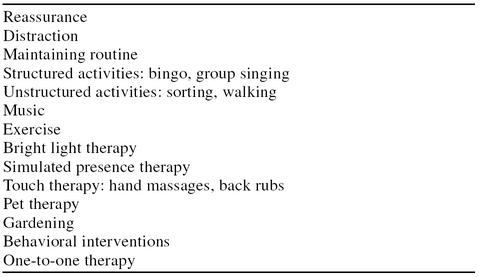
Non pharmacological strategy

What is new?
Bapineuzumab Monoclonal Ab against Beta Amyloid Failed Screening blood test for high risk of MCI, Dementia Found 10 lipid panel. 90% accuracy. May be ready in use in few years. REST – protein represses AD genes (gene regulator) protect neuron

Take Home Message
It is not part of normal aging! It is a terminal disease! Diagnose it early! Look for reversible cause! It’s a clinical diagnosis! AD>DLB> VD>FTD Brain stimulation & exercise helps! Non pharmacological approach first when managing behavioral disturbances! Reduce caregiver burden

Thank You

http://www.alzfdn.org/AboutAlzheimers/symptoms.html

Antidepressants for Dementia associated with depression
1)SSRI Sertraline (zoloft), Citalopram (Celexa), Fluoxetine (Prozac) Escitalopram (Lexapro), Paroxetine (Paxil) 2)Other antidepressants Bupropion (Wellbutrin), Mirtazapine (Remeron), Venlafaxine (Effexor), Duloxetine (Cymbalta) 3)TCA---Not a first choice! reserved for specific group Nortriptyline (Pamelor), Desipramine (Norpramin) 4)Psychostimulants Methylphenidate (Ritalin)
Agitation
Make tasks simpler. Break down complex to smaller simple Allow the person to do as much as possible Provide calm, comforting enviornment. Keep routines Reduce noise Room well lit and comfortable temp Use a snack or activity to distract
Bathing
Use non-slip bath mats grab bars shower seat No need for frequent showers-twice a week Heat bathroom prior to entering Have all supplies ready Do NOT leave person alone in bathroom
Eating
Gentle reminder to eat and drink Eating with others may remind them what to do and how to Finger foods easier and encourge independence Lightweight mug with handle better than glass Offer smaller portions more often
Incontinence
Respect privacy and dignity Remind and/or assist every 2 hours Non-verbal cues: pulling on clothes, agitation Bedside commode Use signs to show way wear easy to remove clothing with elastic waistbands or Velcro closures Drink frequently during day and less in evening
Paranoia
Do not argue Tell you will help look for missing object Keep spares of regularly missed objects Distract with an acitivity
Sleeplessness or sun-downing
Restrict sweets and caffeine later in day more daytime activities-physical exercise discourge afternoon nap Night light and lighted way to bathroom Lock doors Door sensors, motion detectors